Parkinson Disease was originally described in an essay by Dr. James Parkinson titled “An essay on Shaking Palsy” and so it was called for a few decades, the shaking palsy, before being referred to as Parkinson Disease by famous Dr. Charcot. Since original description on clinical symptoms of 6 “people” (3 clinic patients and 3 persons observed while walking on the street) there has been much added to our understanding of history and examination findings in PD and similar diseases.
The next challenge was to understand what goes on in the brain that results in these symptoms and there progression. This was eventually achieved in 1912 when Dr. Fredrich Lewy described “Lewy bodies” inside the neurons in certain regions of the brain. This is a gold standard for confirmation of Parkinson Disease but can only be done on autopsies as Brain biopsies in that part of brain are not safe at all and have never been performed or studied.
We continue diagnosing the patients the same way as it has always been done; by taking history and performing examination albeit with a better understanding of both. Medical imaging evolved over the last 3 decades and is now being extensively used in neurological diseases. The changes in PD however are microscopic and the imaging resolution is nowhere close to pick up on such changes. Routine imaging (esp. Magnetic Resonance Imaging or MRI) is very helpful in ruling out mimics of PD.
Over the last decade, scientists have struggled with finding a way to “mark” the brain in certain way as to differentiate between normal and Parkinson Disease. These markers however are very crude and still are not disease specific. There are few ways to mark the brains, by looking at functional changes by their use of Oxygen, or looking at structural changes by looking at connection between neurons (utilizing techniques to look at flow of water in a certain direction).
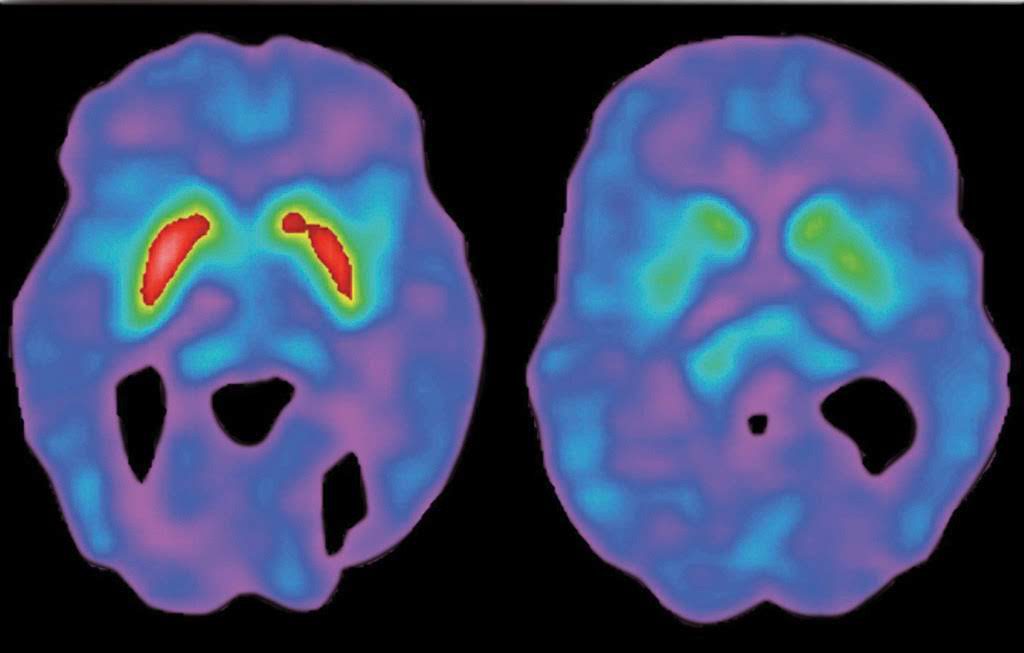
DAT scan or Dopamine Transporter Scan is another novel way of “marking” the brain and it could be thought of as staining a brain and seeing how much of stain is taken up. Then looking at what is normal amount and pattern of staining and comparing it with Parkinson disease as diagnosed by a Movement Disorder expert. It utilizes a specially prepared chemical that has radioactive Iodine bound to it. It changes gradually while giving of x-rays that could be picked up by scanners. This is not a new idea and is commonly used for diagnosis of Thyroid, Breast, Lung, Liver and gall bladder disorders among others. However the challenge was to find the right chemical that will go to brain and mark it in a proper way. The compound being used, binds to an area on neurons called Dopamine Transporter. This is a protein whose job is to pick up some of the released dopamine back to be re-cycled. These are present on the same neurons that make and release dopamine. Therefore marking DAT is a way of counting the number of such neurons and we know that a decline in their numbers is the cause of neurodegenerative parkinsonism.
There are some limitations to it. It cannot differentiate between different reasons of decrease in number of cells so it cannot tell the different types of Parkinsonism apart. It can be affected by other drugs acting in the brain on DAT protein thus giving a falsely low number (e.g. antidepressants). The reading of results which looks like X-ray usually done subjectively and can vary among the reader and can be read as normal in early Parkinson Disease. It is not studied in diagnosing Parkinson disease before onset of clinical symptoms. The comparison with pathological studies (autopsies) that is the gold standard is limited.




